
Serving Greater Boston residents, the Roux-en-Y procedure is recommended for individuals with esophageal injury from conditions such as severe acid reflux and/or Barrett’s esophagus. Bariatric surgeons at Newton-Wellesley Hospital’s Center for Weight Loss Surgery perform laparoscopic Roux-en-Y Gastric Bypass surgery if you are not a candidate for the more common sleeve gastrectomy procedure.
In recent years, better clinical understanding of procedures that combine restrictive (decreasing food intake by reducing the size of your stomach) and metabolic (altering chemicals in your blood to change your perception of hunger and fullness) approaches has increased the options for effective weight loss surgery.
While laparoscopic Roux-en-y gastric bypass was the “gold standard” for 25 years, since 2012 the procedure is done less routinely due to the effectiveness and lower potential complications after a laparoscopic sleeve gastrectomy. Additionally the laparoscopic sleeve gastrectomy may be converted to a SIPS- Duodenal Switch if additional weight loss and treatment of comorbid disease is needed.
The chemical or metabolic change that occurs with bypassing the body of the stomach and the first part of the small intestine results in an early sense of fullness, combined with a sense of satisfaction that reduces the desire to eat.
 How the Surgery Is Done
How the Surgery Is Done
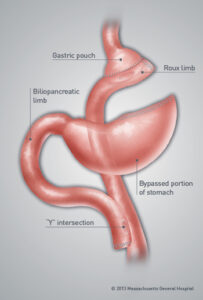
In the Roux-en-Y gastric bypass procedure, stapling creates a small stomach (gastric) pouch. The remainder of your stomach is not removed, but is divided from your stomach pouch and empties into the first part of the intestine which is bypassed.
The outlet from this newly formed pouch empties directly into the lower portion of your jejunum (the middle portion of your small intestine), bypassing the duodenum and delivering nutrients to the end of the small intestine faster thereby providing the metabolic aspect of this operation. The other end is connected into the side of the Roux limb of your intestine, creating the “Y” shape that gives the technique its name.
Advantages
- The average excess weight loss after the Roux-en-Y procedure is generally higher in patients than with purely restrictive procedures.
- One year after surgery, average weight loss is 60-80 percent of excess body weight.
- Studies show that after 10 to 14 years, 50 to 60 percent of excess body weight loss has been maintained by most patients.
- A 2000 study of 500 patients showed that 96 percent of certain associated health conditions studied (back pain, sleep apnea, high blood pressure, diabetes and depression) were improved or resolved.
Risks
- Because your duodenum is bypassed, poor absorption of iron and calcium can result in anemia and osteoporosis. This is a particular concern if you experience chronic blood loss during excessive menstrual flow or bleeding hemorrhoids. Women, who are already at risk for osteoporosis that can occur after menopause, or men with a family history of osteoporosis should be aware of the potential for increased bone calcium loss. This risk is preventable by taking vitamins and supplements and complying with routine follow up annually.
- Bypassing the duodenum has caused metabolic bone disease in some patients, resulting in bone pain, loss of height, humped back, and fractures of the ribs and hip bones. However, these can be managed through proper diet and vitamin supplements.
- You might develop chronic anemia due to vitamin B12 deficiency. The problem can usually be managed with vitamin B12 pills or injections.
- A condition known as “dumping syndrome” can occur as the result of rapid emptying of stomach contents into the small intestine. This is sometimes triggered when too much sugar or fatty foods are consumed. While generally not considered to be a serious risk to your health, the results can be extremely unpleasant and can include nausea, weakness, sweating, faintness, and, on occasion, diarrhea after eating. Some people are unable to eat any form of sweets after surgery.
- In some cases, the effectiveness of the restrictive aspect of the procedure may be reduced if the stomach pouch is stretched.
- The bypassed portion of your stomach, duodenum, and segments of the small intestine cannot be easily visualized using X-ray or endoscopy if problems such as ulcers, bleeding, or malignancy should occur.
Call us at 617-243-3724 to request an appointment.